





HTML
-
回顾性搜集2020年1月30日-2月30日因身体不适(发热、咳嗽、胸闷等)或与武汉NCP患者有密切接触而就诊于武汉科技大学附属普仁医院的患者82例.参考国家卫生健康委员会《新型冠状病毒肺炎诊疗方案(试行第七版)》[1],通过医院影像归档和通信系统(Picture Archiving and Communication Systems,PACS)工作站调取82例患者临床资料,将所有患者分为轻型、普通型、重症型及危重型3组.
纳入标准:①新型冠状病毒核酸检测阳性;②发生临床症状1周内患者. ③未经治疗的初诊患者. ④所有患者均有实验室检查(外周血白细胞计数、淋巴细胞比率、C反应蛋白)结果.
排除标准:就诊前曾治疗的患者.
-
采用美国GE Optima 660 CT扫描仪,患者取仰卧位,吸气后屏气,扫描范围从肺尖到膈顶.采用胸部CT扫描技术.扫描参数:管电压120 kV,管电流50~400 mA,层间距5 mm,层厚0.625 mm.
由2名具有丰富工作经验的放射诊断医师在PACS工作站进行阅片,统计病灶在每个肺叶分布的数量,若病灶同时累及多个肺叶时,则每个肺叶分别各算1个病灶.当2名医师诊断结果不一致时,由第3名高年资医师裁定.
-
所有数据应用SPSS 17.0软件进行统计分析.阳性病灶分布特点为计数资料,采用百分率表示;年龄采用中位数(上、下四分位数)表示.计量资料作正态性检验和方差齐性检验,各组数据均用均数±标准差(x±s)表示,多组间的两两比较采用单因素方差分析,p < 0.05为差异有统计学意义.
1.1. 一般资料
1.2. 检查方法
1.3. 统计学方法
-
CT阳性病灶的影像特点(表 1):共纳入NCP患者82例,男38例,女44例. 82例NCP患者就诊时间均在出现身体不适1周以内或无症状初次就诊.所有患者首诊入院时均做胸部CT检查,其中6例(7.31%)肺内呈阴性表现,76例患者(92.68%)CT呈阳性,其中70例(70/76,92.11%)例患者有肺内GGO[图 1(a)-(c)],6例(7.89%)呈斑片模糊影及其他阴影[图 1(d)];双肺分布GGO为55例[55/70,72.37%],单肺GGO有15例(15/70,19.74%);64例(64/70,91.43%)患者GGO病灶内合并血管束增粗[图 1(a),(b),(d)],6例(6/70,8.57%)未见合并血管增粗[图 1(c)].
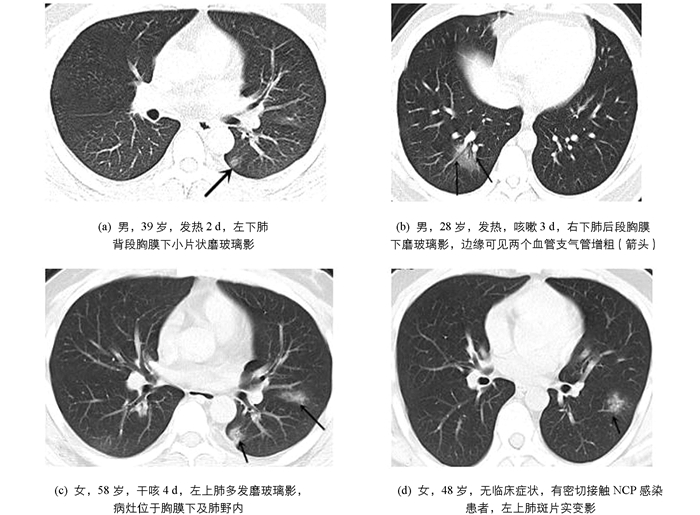
CT阳性病灶部位分布特点(表 1):病灶位于右下肺(70/224,31.25%)及左下肺叶(68/224,30.36%)多见;病灶分布于胸膜下及肺野外带58例(58/70,82.86%),其他部位分布12例(12/70,17.14%).
-
发病早期临床各型病灶累及肺叶数量(表 2):82例NCP患者中,属于轻型患者10例,病灶累及肺叶28个;普通型60例,病灶累及肺叶149个;重型及危重型患者12例,病灶累及肺叶37个.临床各型患者发病早期病灶累及肺叶数量比较差异无统计学意义(F=2.317,p > 0.05),两两间比较差异无统计学意义.
临床表现:82例NCP患者中发热60例(73.17%),咳嗽52例(63.41%),多为干咳(44例,53.66%),肌肉酸痛27例(32.93%),腹痛、胸闷、恶心及纳差各10例(12.20%),无症状7例(8.54%).
2.1. 影像表现
2.2. 临床资料
-
新型冠状病毒肺炎(NCP)是严重急性呼吸综合征冠状病毒2(SARS-CoV-2)感染的疾病,主要经呼吸道飞沫和接触传播.气溶胶和消化道等传播途径尚待明确,NCP发病率高,传播迅速,是一种新发的具有较强传染性的肺部疾病[2-4]. NCP须由核酸检测或基因测序作为确诊的关键指标.然而,由于核酸检测或基因测序样本采集、运输和试剂盒性能受到诸多因素影响,导致检测不便,且核酸检测也存在假阴性可能.胸部CT作为诊断肺炎的常规影像学手段,具有操作简便、诊断速度快等优点. Ai等[5]发现,根据核酸阳性结果,胸部CT提示NCP的敏感性为97%(95%CI,95%~98%,580/601),胸部CT对NCP的诊断具有较高的敏感性,可作为目前流行区NCP检测的主要工具. 2020年3月4日,国家卫生健康委也发布了《新型冠状病毒肺炎诊疗方案(试行第七版)》,特别强调了CT影像学对于湖北防控策略“早诊断、早隔离”的重要价值.本文着重分析NCP患者早期胸部CT影像表现及临床特点,尝试尽早诊断该病,这对于疾病治疗及控制疫情具有重要意义.
磨玻璃影(GGO)是在CT肺窗上表现为肺透亮度稍下降、肺密度稍增高的一种阴影,支气管及血管边缘仍能显示,纵隔窗GGO不显示. GGO形成原因为[6-7]:①肺泡的容积减少及含气量减少,肺泡腔内气体被渗出液、血液、炎性细胞或无定型物质置换;②肺组织间质及肺泡壁增厚,因水肿、肿瘤增生、纤维化和非癌性肉芽肿沉积而增厚;③肺栓塞及肺血管炎所致肺血流灌注相对增加.肺部GGO可以为良性病变,如局灶性间质纤维化、炎症、感染和出血,也可以是肺腺癌及浸润前病变[8].
GGO表现多种多样,间质性肺炎表现为弥漫性GGO,多伴有蜂窝状透亮影及网格影.双肺坠积性效应有按重力分布特点,多表现在双下肺近背侧弧分布形.心源性肺水肿患者多有心、肾功能障碍,且多为双侧、对称分布,伴有小叶间均匀增厚.
我们发现,NCP病灶呈胸膜下GGO[58(58/70,82.86%)]分布多见,可能是因为SARS-CoV-2直接侵犯终末细支气管远端的肺腺泡,导致肺泡损伤[9]并侵犯肺泡周围血管,引起胸膜下血管炎,导致肺泡内炎性渗出物增加,空气含量减少,周围肺间质及肺泡壁增厚,形成了大量胸膜下GGO及血管束增粗. Heitzman等[10]认为,肺分为周围的肺皮质和中央的肺髓质.周围的肺皮质内的肺小叶形状为扇形或弧形排列,肺外周有丰富的毛细血管及有换气功能的肺泡,易引发炎症反应,NCP患者双肺胸膜下病灶正好符合这种肺小叶解剖上的差异.而NCP患者早期病灶渗出不明显,多不伴胸腔积液及大片实变影.
在本组病例中,我们发现双肺GGO以右下肺(70/224,31.25%)及左下肺叶(68/224,30.36%)为主,有文献认为双下肺为主,右肺中叶受累相对少见[11],这可能与肺内气流分布有关,具体原因还有待研究.
临床各型患者发病早期病灶累及肺叶数量相比较差异无统计学意义(F=2.317,p > 0.05).武汉大学中南医院WANG等[12]报告的138例NCP住院患者中,36例重症患者有明显的基础疾病,包括高血压病(58.3%)、糖尿病(22.2%)、心血管疾病(25%)、脑血管疾病(16.7%).陈雷等[13]发现患者血清中白介素-2受体(IL-2R)、白介素-6(IL-6)水平与病情严重程度有明显的相关性.这些研究可能说明,新冠肺炎的严重程度可能与患者基础疾病有关,也可能与个体对疾病的反应有关,而与早期病灶数量累及肺叶的多少没有关系.
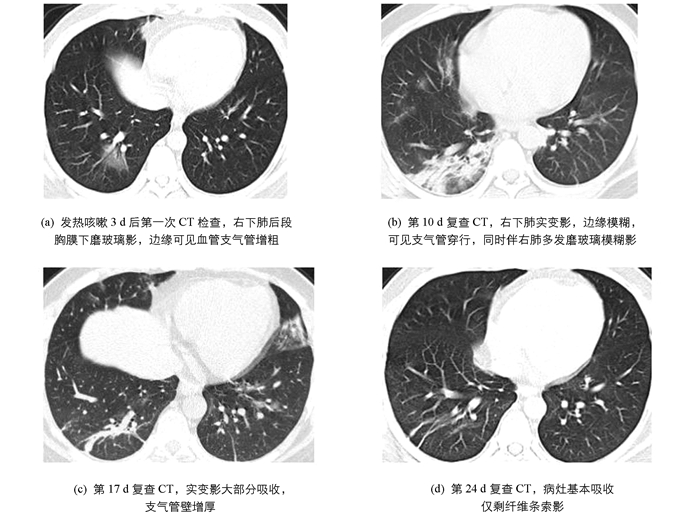
病情发展预测:据中华医学会放射学分会专家推荐意见[14],将NCP的CT表现分为早期、进展期和重症期.早期[图 2(a)]即为单发或多发GGO;进展期[图 2(b)]病变范围进一步扩大、分布区域增多,可见实变影及空气支气管征伴小叶间隔增厚;重症期为双肺弥漫性实变,部分呈“白肺”表现.绝大多数患者经过治疗,病灶范围缩小,密度减低,实变逐渐消失,部分残留条索灶[图 2(c),(d)].
目前也是流感的高发季节,在当前特殊时期若发现肺内有GGO、实变、结节等影像表现,需要排除病毒性肺炎、重症急性呼吸窘迫综合征(SRARS)、支原体及细菌感染等.甲型流感病毒肺炎多是单侧或双侧局灶或多发GGO,伴或不伴实变,常沿支气管血管束分布或胸膜下分布[15-16],NCP早期可表现为小GGO或小片磨玻璃影内见增粗血管影,可能有助鉴别.腺病毒肺炎常见于儿童,胸部CT表现为双肺弥漫或局限性GGO,伴或不伴实变. SRARS与NCP致病病毒同属冠状病毒,两者致病机制和影像学表现高度相似,单纯影像学难以鉴别,最终需借助病原学检测.支原体肺炎儿童和青少年常见,最常见的症状有发热、刺激性干嗽.胸部CT呈沿支气管血管束分布为主的气腔实变及GGO,呈自肺门向肺野外围伸展的大片扇形阴影,可见支气管壁增厚及细支气管“树芽征”与肺门及纵隔淋巴结肿大,实验室检查支原体抗体阳性[17].细菌性肺炎多无上呼吸道感染前驱症状,咳脓性痰,血性痰或铁锈色痰,白细胞数增高,影像学多表现为肺叶或段实变影,抗生素治疗效果好.
总之,NCP有其特有的影像学征象,CT阳性患者早期主要表现为胸膜下和/或双肺野外带磨玻璃影及斑片影,常合并灶内血管束增粗,临床有发热、咳嗽、肌肉酸痛等症状,实验室检查白细胞计数减少、淋巴细胞比例降低,C反应蛋白上升,且有流行病学史时需考虑NCP.确诊NCP的金标准为核酸检测阳性,对于核酸检测阴性及CT检查呈阴性的患者,也不能大意,临床应及时复查,以便早发现、早诊断、早隔离、早治疗.
 DownLoad:
DownLoad: